
Severe Bradycardia in COVID-19: Moving Beyond Typical Respiratory Symptoms
Introduction. A 61-year-old woman presented to the emergency department with a 1-week history of cough, worsening shortness of breath, and dizziness.
History. The patient had a history of hypertension, type 2 diabetes, asthma, reactive airway disease, hyperlipidemia, and intermittent migraine headaches, but had no known cardiac disease or significant history of bradycardia. Her home medications included propranolol extended release (60 mg daily), metformin extended release (ER) (500 mg every morning), montelukast (10 mg daily), rosuvastatin (10 mg daily), amitriptyline (25 mg nightly), aspirin (81 mg daily), aspirin-acetaminophen-caffeine (250-250-65 mg as needed for migraine headaches), and naproxen (500 mg bid as needed for headaches).
Upon presentation, the physical examination revealed woman was diaphoretic and in mild respiratory distress with bilateral lung rales and bradycardia. Her extremities were cool and clammy, but the rest of the examination was unremarkable. The patient presented with sepsis, including hypotension with a blood pressure of 91/43 mmHg. Unexpectedly, she was bradycardic, with heart rates in the 50s.
Diagnostic testing. The patient was initially diagnosed with bradycardia based on a physical examination. The right radial pulse was palpated, and the patient was found to have a heart rate in the 40s. To confirm the diagnosis of bradycardia, the patient was then given an electrocardiogram (EKG). The EKG results confirmed sinus bradycardia with no evidence of heart block or any other electrical abnormality (Figure 1). The patient had no prior history of arrhythmias, nor history of orthostatic or syncopal episodes. Finally, the patient had no evidence of myositis or pericarditis.
In the ED, she tested positive for COVID-19 through rapid antibody testing and chest X-ray showed pneumonia consistent with COVID-19 infection. The patient was then admitted to the hospital with a complete blood count significant for leukocytosis at 16 k/uL but was otherwise unremarkable. The patient exhibited a normal anion gap. Importantly, she had never exhibited bradycardia on propranolol before her COVID-19 infection. Moreover, propranolol was discontinued upon admission, and her bradycardia persisted beyond any possible residual beta-blocker activity. Propranolol ER has a half-life of around 8 to 11 hours and the patient continued to have significant bradycardia for nearly one week after propranolol was discontinued.
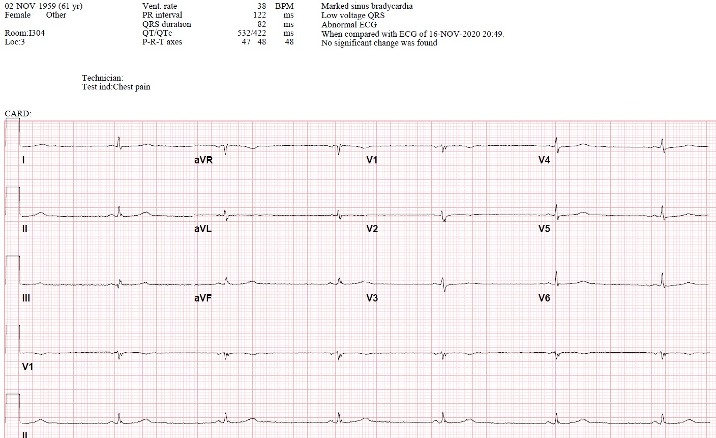
Figure 1: Marked sinus bradycardia after COVID-19 diagnosis. Ventricular Rate: 38 bpm.
Differential Diagnoses: When the patient first presented, COVID-19 induced bradycardia was not at the top of the differential. The more likely possibility was that her bradycardia was secondary to the patient’s prescribed propranolol. However, this was eventually ruled out because her bradycardia persisted far beyond the period of any possible residual beta blocker activity. Another potential differential diagnosis was various forms of heart block. However, formal EKG showed no evidence of first, second, or third degree heart block. Finally, the patient having sinus bradycardia at baseline was ruled out after a thorough review of her medical chart revealed no history of significant bradycardia.
Treatment and management. The patient received the standard of care for COVID-19 pneumonia at the time, which included a course of remdesivir and dexamethasone. Remdesivir inhibits viral replication through inhibition of RNA polymerase1. Despite potential for bradycardia as an adverse effect, remdesivir was deemed beneficial in this case after a risk-benefit assessment1. Her propranolol was discontinued upon admission, and norepinephrine was initiated, then titrated to maintain a mean arterial pressure of greater than 65 mmHg to address her orthostatic hypotension, bradycardia, and moderate to severe hypotension. Additionally, given evidence of early septic shock, blood cultures were obtained followed by simultaneous intravenous antibiotics and IV fluids.
Outcome and follow-up. The patient fully recovered from her COVID-19 pneumonia, was taken off norepinephrine after 3 days, and was discharged on day 7 with a heart rate of 62 bpm after being monitored on telemetry for 24 hours without any additional significant bradyarrhythmia’s. Before discharge, the patient was instructed to continue to hold her propranolol indefinitely. Although she was not discharged with a Holter monitor, she was told to call should she develop symptoms of lightheadedness or dizziness, and this would be ordered accordingly. Her EKG at a 2-month follow up (Figure 2) showed normalization of her heart rate at 75 bpm. At this follow-up, the patient decided not to pursue any further electrophysiology studies.
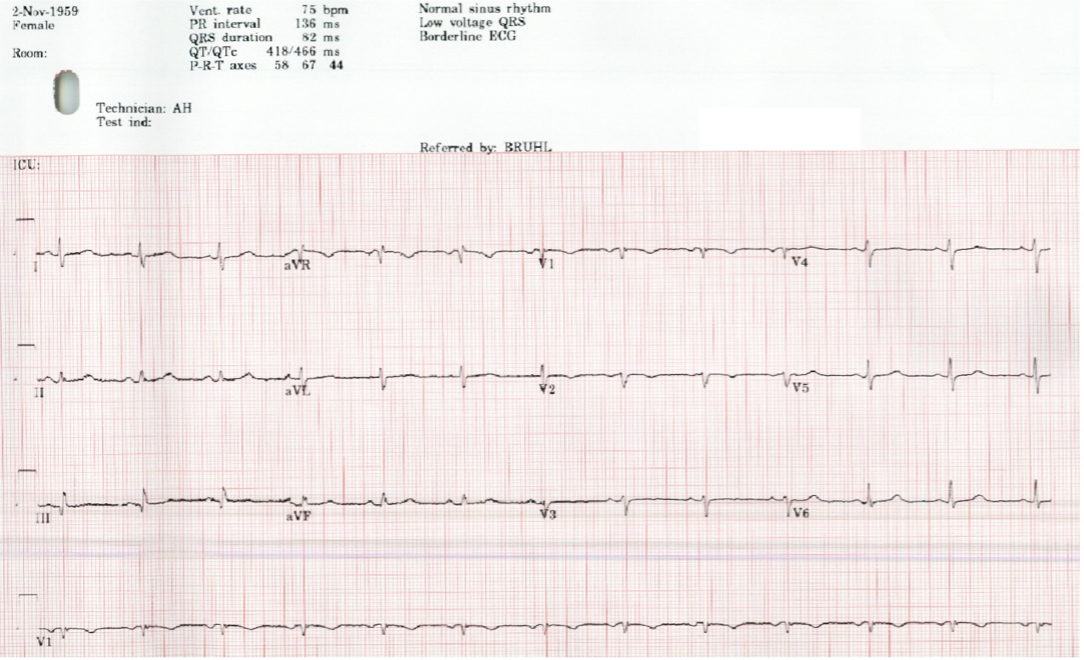
Figure 2: EKG of the patient following treatment for SARS-CoV-2 induced bradycardia. Ventricular rate: 75 bpm.
Discussion. Although infrequent, instances of patients with COVID-19 infection presenting with moderate to severe bradycardia have been documented in a handful of case reports, but the mechanism of action is not yet well understood. One study found that 10 out of 113 patients admitted to intensive care units for severe COVID-19 exhibited sinus node bradycardia with a median heart rate of 36 bpm2, resulting in a prevalence of 8.84%. This could help explain the notably worse survival rates among patients with cardiac disease compared to those without such history.
Before the 2020 COVID-19 pandemic, this disease was quite rare and not extensively researched; therefore, the pathophysiology behind COVID-19-induced bradycardia remains unclear. However, infection-induced bradycardias from other diseases are better understood and could provide some potential hypothesis to consider. For instance, American trypanosomiasis (commonly known as Chagas disease), which is caused by the protozoan Trypanosoma cruzi, is believed to induce sinus bradycardia by causing an abnormality in the sinus node's innervation, based on experimental research3. Another infection, borreliosis (known as Lyme disease), caused by the bacteria Borrelia burgdorferi, can lead to atrioventricular conduction irregularities and ultimately severe bradycardia and/or complete heart block when left untreated.4 Another study reviewed 15 viruses, such as influenza, Zika, and dengue, which have proven to induce arrhythmias.5 These viruses appear to have this effect by either altering cardiac ion channels, infecting endothelium, or by invading myocytes. COVID-19 may have a similar mechanism of action.5
Specific to COVID-19, some researchers have proposed that COVID-19 may spur the immune system into a cytokine storm, producing inflammatory cytokines like Interleukin-6 (IL-6).6 IL-6 can increase vagal tone, activate the parasympathetic nervous system, and subsequently decrease heart rate. Additionally, inflammatory cytokines may target cardiac pacemaker cells, altering heart dynamics7 and having an inhibitor effect on sinus node conductance.8 Cardiac cells express angiotensin-converting enzyme 2—a known receptor for COVID-19—and its interaction with COVID-19 could induce cardiac tissue inflammation and modify heart rate.6
Conclusion. While the pathophysiology behind SARS-CoV-2 induced bradycardia is not yet fully understood, cases like the one described here underscore the need for a prepared and effective treatment approach. More invasive interventions, like pacemaker implantation, might be required, depending on the individual circumstances. Whether they are cardiologists, emergency physicians, general practitioners, or other specialists, all physicians must be vigilant about the myriad of cardiac symptoms COVID-19 can induce. Considering the reality that COVID-19 infections are likely to be with us for many years to come, reporting and recognition of this important and potentially life-threatening disease sequela is important for the medical community worldwide.
AUTHORS:
Steven R. Bruhl, MD, MS, FAAC1 • Andrew J. Slembarski, MD2
AFFILIATIONS:
1MercyHealth Tiffin Cardiology Specialists, Tiffin, OH
2Anesthesiology Residency, The Ohio State University, Columbus, OH
CITATION:
Bruhl SR, Slembarski AJ. Severe bradycardia in COVID-19: moving beyond typical respiratory symptoms. Consultant. Published online XX. doi:10.25270/con.2024.12.000003
Received September 20, 2023. Accepted May 14, 2024.
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS:
None.
CORRESPONDENCE:
Steven R. Bruhl, MD, MS, FAAC, MercyHealth Tiffin Cardiology Specialists, 45 St. Lawrence Drive, Tiffin, OH 44883 (steven_bruhl1@mercy.com)
References
1. Kanagala SG, Dholiya H, Jhajj P, et al. Remdesivir-induced bradycardia. South Med J. 2023;116(3):317–320. doi:10.14423/SMJ.0000000000001519
2. Larue J, Jode P, Timsit J, Franchineau G, Extramiana F, Algalarrondo V. Severe bradycardia in criticaly ill patients with COVID-19. Circulation. 2020 ;142(3). doi: 10.1161/circ.142.suppl_3.17124
3. Caeiro T, Iosa D. Chronic Chagas' disease: possible mechanism of sinus bradycardia. Can J Cardiol. 1994;10(7): 765–768.
4. Grella BA, Patel M, Tadepalli S, Bader CW, Kronhaus K. Lyme carditis: a rare presentation of sinus bradycardia without any conduction defects. Cureus, 2019;11(9): e5554. doi:10.7759/cureus.5554
5. Lee PY, Garan H, Wan EY, Scully BE, Biviano A, Yarmohammadi H. Cardiac arrhythmias in viral infections. J Interv Car. Electrophysiol. 2023;66(8):1939-1953. doi:10.1007/s10840-023-01525-9
6. Ikeuchi K, Saito M, Yamamoto S, Nagai H, Adachi E. Relative bradycardia in patients with mild-to-moderate coronavirus disease, Japan. Emerg Infect Dis. 2020;26(10):2504-2506. doi:10.3201/eid2610.202648
7. Amaratunga EA, Corwin DS, Moran L, Snyder R. Bradycardia in patients with COVID-19: a calm before the storm?. Cureus, 2020;12(6):e8599.
doi:10.7759/cureus.8599
8. Capoferri G, Osthoff M, Egli A, Stoeckle M, Bassetti S. (2020). Relative bradycardia in patients with COVID-19. Clin Microbiol Infect. 2021;27(2):295-296. doi:10.1016/j.cmi.2020.08.013