
Doubt It’s Gout? A Case Report of Acute Gout Flare in the Setting of Hypouricemia
Introduction. A 75-year-old male presented to our sports medicine clinic with acute-on-chronic, erythematous lateral ankle pain of 3 months’ duration.
History. The patient denied any injury or trauma to the foot or ankle. Instead, the pain was described as crampy and localized to the distribution of the peroneal brevis muscle tendon. The pain was present intermittently for several days even at rest and was exacerbated with physical activity. When the pain was at its most severe, the patient was unable to bear weight on the left foot.
At 3 months prior to presentation, he was diagnosed with peroneal tendonitis in the emergency department (ED) and was treated with a methylprednisolone dose pack. He was unable to take nonsteroidal anti-inflammatory drugs (NSAIDs) at that time due to his having undergone a gastrectomy 8 weeks prior for neuroendocrine tumor. Oral steroids were also contraindicated during this post-gastrectomy window. He followed up with physical therapy twice per week for 6 weeks, with no resulting improvement. The patient presented to our clinic seeking NSAIDs or oral steroids for pain relief.
Upon examination, the left ankle was intensely swollen and erythematous with significant pain around the lateral malleolus. Pes cavus was noted bilaterally with poor calcaneal varus movement when standing on his toes. There was no tenderness to palpation over the lateral leg compartment.
Diagnostic testing. Point-of-care ultrasonography showed tenosynovitis of the peroneal brevis tendon (Figure 1) along with a joint effusion (Figure 2). No clear tophi or double contour sign was noted. A chart review revealed a previous diagnosis of gout. The patient had been on allopurinol 300 mg per day for more than 1 year and was using 0.4 mg colchicine daily for treatment of flare-ups. A recent uric acid level of 3.4 mg/dL was noted. The goal for gout treatment is to have a uric acid below 6, so the patient was seemingly well-controlled. Still, the patient was referred to rheumatology on the clinical suspicion of acute gout attack.
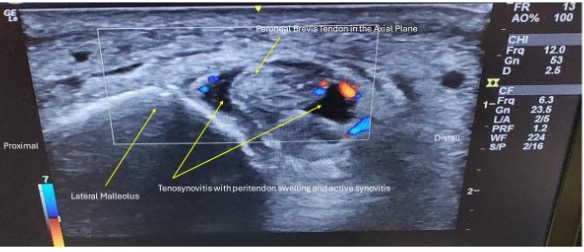
Fig. 1. Short axis view of the peroneal brevis tendon demonstrated intense hyperemia and swelling indicative of tenosynovitis.
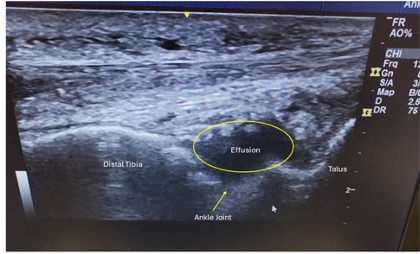
Fig. 2. Long axis view of the ankle joint demonstrating effusion.
Differential Diagnoses. Among the diagnoses considered, one possibility was peroneal tendonitis. This was considered to be likely due to the location of the pain and the clinical diagnosis received in the Emergency Department weeks prior. However, after weeks of physical therapy and methylprednisolone dose pack treatment with absence of symptomatic improvement, this lowered peroneal tendonitis on the differential. Also considered was osteoarthritis of the ankle due to location of the pain over the lateral malleolus and absence of symptomatic improvement with conventional treatments. However, due to the absence of joint space narrowing or osteophytes on imaging, this was rejected from the differential. Similarly, atraumatic tendon avulsion was considered as a possible etiology, but imaging showed an intact peroneal brevis muscle tendon. Septic arthritis was considered due to the erythema and symptomatology. The site was not noticeably warm to the touch on exam, and the patient did not have a fever, leukocytosis, or other signs of systemic response to infection. Malignancy was also considered for these reasons. Finally, acute gout flare was considered due to the patient’s prior history of gout, but suspicion was low due to chronic allopurinol use. Rule-out of septic arthritis, malignancy, and acute gout flare requires joint aspiration.
Treatment and management. The patient was referred to rheumatology, where the lateral talocrural joint was aspirated, and monosodium urate crystals were identified. The patient was diagnosed with acute gout flare. Allopurinol dosage was increased from 300 mg to 400 mg daily, and colchicine was restarted at 0.4 mg daily. His pain resolved completely in 48 hours. Serum urate was scheduled to be rechecked at the 2-week and 3-month marks.
Outcome and follow-up. At the patient’s 2-week follow-up visit, his serum urate was found to be increased to 4.1 mg/dL, and no changes to his serum urate lowering therapy were made at that time as he was asymptomatic. At the patient’s 3-month follow-up, his serum urate was still increased at 4.8 mg/dL. He remains pain free since this change to his medications.
Discussion. Acute gouty arthritis is often diagnosed without joint fluid analysis using the primary care diagnostic rule (PCDR), which includes clinical presentation factors such as rapid onset (within 1 day), first metatarsophalangeal joint erythema and pain, a history of cardiovascular disease, male sex, and plasma uric acid levels greater than 5.88 mg/dL.1 However, as this case report demonstrates, not all acute gout flares adhere to these diagnostic criteria. The absence of an elevated serum urate level can cause clinicians to deprioritize gout from their differential diagnosis and skip joint aspiration, missing the opportunity for accurate diagnosis.
Several physiologic, pharmacologic, and pathologic factors can contribute to a gout flare, even in the setting of low serum urate levels. Although cases of gout flare associated with acute decreases in serum urate levels have been documented,2,3 there is sparse documentation of acute gout attacks in the setting of chronically low serum urate levels in patients on long-term allopurinol treatment.
The gold standard for diagnosis of gout is synovial fluid aspiration and examination using compensated polarized light microscopy to detect monosodium urate crystal. However, primary care and emergency medicine physicians often rely on clinical algorithms such as the PCDR to avoid inflicting increased discomfort through diagnostic aspiration of an already severely painful joint. In this case, the patient's use of urate-lowering therapy, low serum urate level, and the location of pain in the ankle led to the diminished suspicion of a gout flare at the time of his ED visit.
Although classic literature4 emphasizes gout locale in the first metatarsal-phalangeal joint, other common locations for gout flare that are not listed in the PCDR include midfoot, ankle, knee, elbow, wrists, and fingers. The current consensus goal in serum urate lowering therapy for effective long-term gout management is serum urate below 5 mg/dL. An association between baseline serum urate levels and clinical manifestations of gout has long been assumed in the clinical guidelines for treatment of the disease. A recent study from McCormick et al. showed findings suggestive of confirmation that in patients with a history of gout, higher serum urate levels at baseline are associated with an increasing risk of subsequent gout flares and rates of hospitalization for recurrent gout.5
Several studies have highlighted cases where low serum urate levels have been associated with gout flares.2,3 For example, one case reported a patient who developed gout after renal transplantation, despite urate levels as low as 2.7 mg/dL.2 Another case involved a patient receiving TPN, which led to a serum urate level of 4.6 mg/dL at the time of joint aspiration.3 These examples challenge the assumption that elevated serum urate is a prerequisite for diagnosing gout.
Abrupt decreases in serum uric acid levels, even in patients receiving allopurinol or other urate lowering therapy (ULT), can trigger acute gout flares.6 This phenomenon underscores the importance of using prophylactic NSAIDs or colchicine when starting ULT or adjusting doses. Patients are also at risk for flares even a few months after reaching serum uric acid goal due to mobilization from joint spaces, and flares should be expected to continue until there has been a sustained period with serum urate remaining below 6.0 mg/dL.7
Other complicating factors include the presence of tophi or the effects of adrenocorticotropic hormone (ACTH). Approximately 20-30% of patients with acute gout flare will have low uric acid levels due to the uricosuric effects of ACTH, and tophi can contribute to persistent mobilization of uric acid within joints, potentially causing ongoing flares even when serum uric acid levels are low.7
Finally, other serious etiologies for an acutely warm, non-traumatic, tender joint include infection and malignancy, both of which warrant joint aspiration. In this case, a definitive diagnosis was delayed due to reliance on PCDR and the perception of patient comfort, resulting in unnecessary pain for the patient. Had chronic gout been appropriately considered in the differential diagnosis during the initial ED evaluation—regardless of serum urate levels—his pain could have been alleviated sooner. Point-of-care ultrasonography could have also revealed the joint effusion, prompting further diagnostic evaluation and potentially reducing the delay in diagnosis.
This case provides another example of acute gout despite low uric acid levels and exemplifies the role of ultrasound as well as the axiom of a hot swollen joint that should be aspirated.
Conclusion. Atraumatic painful joints with effusion require a definitive diagnosis. Although patient comfort is a concern, clinicians should not let their perception of patient comfort restrict their use of joint aspiration as a method of evaluation. Similarly, while the use of algorithms such as the PCDR can help guide further workups, these should not preclude the use of gold standard diagnostics for definitive diagnosis. The PCDR has proven effective in ruling out acute gout flare, with a negative predictive value of 0.87. However, its positive predictive value is lower (0.64), and its specificity is only 28%. This demonstrates that while the PCDR is useful for excluding gout, it is less reliable in confirming the diagnosis, especially when serum urate levels are not elevated.1 Rapid, accurate diagnosis can prevent the need for multiple visits, months of unnecessary pain, and reduce potential damage from delay of diagnosis.
AUTHORS:
Brock A. Preheim, MS1 • Jeffrey C. Leggit, MD, CAQSM2
AFFILIATION:
1School of Medicine, University of Tennessee Health Science Center, Memphis, TN, 38163, United States of America
2Department of Family Medicine, Uniformed Services University School of Health Sciences, Bethesda, MD, 20814, United States of America
CITATION:
Preheim BA, Leggit JC. Doubt it’s gout? A case report of acute gout flare in the setting of hypouricemia. Consultant. Published online December 20, 2024. doi: 10.25270/con.2024.12.000006.
Received July 8, 2024. Accepted September 27, 2024.
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS:
None.
CORRESPONDENCE
C. Leggit, MD, CAQSM, Department of Family Medicine, Uniformed Services University School of Health Sciences - Bethesda, MD, 20814 (jeff.leggit@usuhs.edu)
References
- Janssens HJEM, Fransen J, van de Lisdonk EH, van Riel PLCM, van Weel C, Janssen M. A diagnostic rule for acute gouty arthritis in primary cCare without joint fluid analysis. Arch Intern Med. 2010;170(13):1120-1126. doi:10.1001/archinternmed.2010.196
- Juraschek SP, Kurano T, Rosen A, Gelber AC. Acute gout after renal transplantation with notable hypouricemia. Am J Med. 2013;126(10):e5-6. doi:10.1016/j.amjmed.2013.04.008
- Moyer RA, John DS. Acute gout precipitated by total parenteral nutrition. J Rheumatol. 2003;30(4):849-50.
- Hadler NM, Franck WA, Bress NM, Robinson DR. Acute polyarticular gout. Am J Med. 1974;56(5):715.
- McCormick N, Yokose C, Challener GJ, Joshi AD, Tanikella S, Choi HK. Serum urate and recurrent gout. JAMA. 2024;331(5):417-424. doi:10.1001/jama.2023.26640
- Burns CM, Wortmann RL. Latest evidence on gout management: what the clinician needs to know. Ther Adv Chronic Dis. 2012;3(6):271-86. doi:10.1177/2040622312462056
- Schlesinger N. Difficult-to-treat gouty arthritis: a disease warranting better management. Drugs. 2011; 71(11):1413-39. doi:10.2165/11592290-000000000-0000