
Psoriasis: A Review of Diagnosis and Treatment in the Primary Care Setting
ABSTRACT: Psoriasis is a ubiquitous chronic inflammatory skin disease that occurs most often in adults, with men and women affected with equal prevalence. Psoriasis is frequently encountered in the primary care setting. This article reviews the presentation of psoriasis subtypes and their diagnosis, along with the numerous topical and systemic treatment options and their risks and benefits. Suggestions and recommendations are offered about specialist referral of patients with psoriasis, surveillance of the condition, and the management of associated comorbidities.
KEYWORDS: Psoriasis, primary care, corticosteroids, vitamin D analogues, retinoids, phototherapy, laser therapy, methotrexate, acitretin, apremilast, biologic therapies
Psoriasis is a chronic inflammatory skin disease that affects tens of millions of people worldwide. In the United States, the prevalence of psoriasis ranges from 0.5% to 4.6%.1 It has an equal male to female distribution, and it is seen mostly in the adult population. Psoriasis is a condition that is often encountered in the primary care setting. This article reviews the disease presentation, diagnosis, and treatment options and offers suggestions and recommendations about referral to a dermatologist, surveillance, and the management of comorbidities.
Psoriasis manifestations can range from a few spots on the elbows, knees, or scalp to severe systemic involvement. Psoriasis is a chronic disease characterized by cycles of remissions and exacerbations.
Psoriasis is not only a cosmetic nuisance. It can cause significant psychological dysfunction, evidenced by patients having reported impaired physical and mental functioning comparable with that seen in other chronic conditions such as cancer, diabetes, depression, and hypertension.2 Some studies have found that psoriasis vulgaris may have a considerable negative impact on patients’ quality of life, similar to that of angina or hypertension.3 Additionally, many persons with psoriasis report feeling stigmatized and isolated.2,4
Psoriasis Definition and Subtypes
Psoriasis is a chronic skin condition that is associated with varying degrees of systemic involvement. Psoriasis affects the nails and joints in 5% to 20% of cases.5 It predisposes patients to an increased risk of other conditions, including arthritis, metabolic syndrome, cardiovascular disease, insulin resistance, hypertension, and other diseases that follow endothelial dysfunction and atherosclerosis formation.
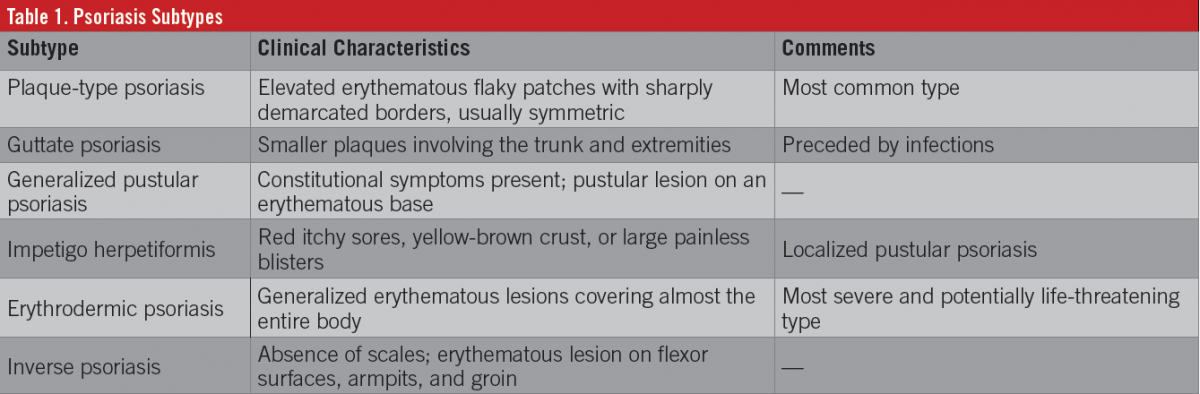
The most common subtype of psoriasis in the United States is plaque-type psoriasis, affecting approximately 80% of patients diagnosed with psoriasis. Plaque psoriasis has a predilection for the hairy scalp, the extensor surfaces of the elbows and knees, and the gluteal cleft.6 Other types of psoriasis occur less frequently and may have a different distribution and characteristic lesion (Table 1).
Pathophysiology
Psoriasis is an inflammatory disease that has genetic overlap with rheumatoid arthritis and Crohn disease. Multiple genetic and environmental factors play a role in the development of psoriasis. More than 40 genetic mutations have been implicated in the development of psoriasis, including mutations to IL36RN, AP1S3, CARD14, KLRC2, LNPEP, LCE3B, LCE3C, TRAF3IP2, MTHFR, and ZNF750.
Activated T cells migrate to and infiltrate affected areas, releasing interferon-γ, interleukin-2 (IL-2), and tumor necrosis factor-α (TNF-α).1 Other players involved include natural killer T cells, the T helper 17 cell, dendritic cell overproduction and secretion of IL-23, activated macrophages, and T regulatory cells.
The end result is inflammation and hyperproliferation of keratinocytes, whose migration time from the basal layer to the corneal layer is reduced from 20 to 30 days to 3 to 5 days.5
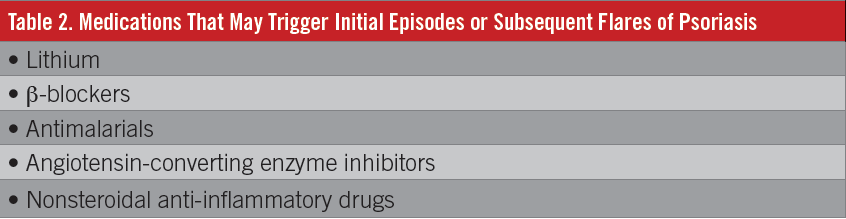
Infections, such as with β-hemolytic streptococci and human immunodeficiency virus, have been associated with the development of psoriasis, be it a causal or incidental association. Whether infection plays a crucial role in the development of psoriasis or whether it is directly involved in the vascular damage that occurs with psoriasis has not been extensively studied.7 Stress, tobacco use, infections, alcohol use, hormones, skin trauma, and possibly medications have been implicated in triggering first occurrences or subsequent outbreaks of psoriasis (Table 2).8,9
Diagnosis
Psoriasis usually can be diagnosed based on the physical examination. Laboratory and histopathologic confirmation rarely are needed. The skin lesions of psoriasis are sharply demarcated, red, scaly plaques with variable patterns and body distribution. Commonly affected areas include the scalp, the extensor surfaces of the elbows and knees, the umbilicus, the gluteal cleft, and the nails (Figure 1). If adherent scale is removed, pinpoint bleeding may be evident (the Auspitz sign).

The differential diagnosis of psoriasis includes tinea infections, eczema/atopic dermatitis, seborrheic dermatitis, systemic lupus erythematosus, and cutaneous T-cell lymphoma (Table 3).

Associated Risks
Joint involvement occurs in 15% to 30% of patients.5 Psoriatic arthritis usually involves the distal interphalangeal joints in a symmetric fashion. Half of patients with joint involvement develop early, rapidly progressive joint damage (11% annual erosion rate) in the first 2 years of disease duration.10 Because skin disease generally occurs before joint pain, patients being seen for psoriasis should be monitored for the development of joint symptoms. A sensitive screening test for psoriatic arthritis is asking patients about the presence of joint pain, joint stiffness (especially morning stiffness), and back pain.
Systemic, proinflammatory conditions such as psoriasis predispose patients to increased cardiovascular risks secondary to accelerated atherosclerosis formation and premature vascular damage.11 Therefore, these patients should receive age-appropriate surveillance of blood pressure, weight, cholesterol level, liver function, glucose level, and renal function.
Psoriasis Treatment
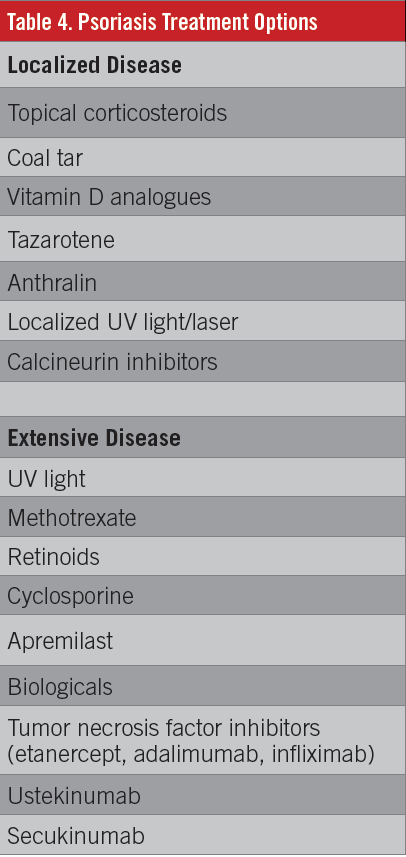
The first step of treatment of a patient with psoriasis is to address and treat any psychosocial concerns as necessary. Figure 2 presents a psoriasis treatment algorithm. The National Psoriasis Foundation (NPF, www.psoriasis.org) offers a host of resources for addressing these needs. The patient then is screened for any joint involvement and is referred to a rheumatologist if any early joint involvement is suspected. The next step is to determine whether the patient has localized lesions that are amenable to topical treatment alone (often termed mild to moderate psoriasis) or more extensive involvement for which topical treatment alone is not practical (moderate to severe psoriasis). Patients with localized lesions usually are treated with topical preparations and possibly localized ultraviolet (UV) phototherapy, whereas patients with extensive disease manifestations may require phototherapy or systemic agents (along with topical treatment of the worst lesions) (Table 4).

Localized psoriasis. Topical corticosteroids are the first-line treatment for localized psoriasis and have good efficacy in the treatment of mild-to-moderate psoriasis vulgaris. Topical corticosteroids vary from low potency such as hydrocortisone, to medium potency such as triamcinolone, to high potency such as betamethasone dipropionate (and ultrahigh-potency clobetasol). Even with rising prices for generic products, these agents generally are still low-cost formulations. Low-potency formulations are used for the face and genital area, while higher-potency corticosteroids are used for thicker plaques on the body and scalp.
Topical corticosteroids can be used in combination with other treatments, but making the treatment too complicated can compromise patient adherence. Newer, less-messy formulations such as foams and sprays can contribute to increased efficacy by improving ease of use. Prescribers should monitor for adverse effects such as skin atrophy and the more serious but rare hypothalamic-pituitary-adrenal axis suppression. Other common skin reactions are telangiectasia and acne exacerbation at the application site. Few patients experience skin hypopigmentation, hyperpigmentation, or secondary skin infections.
The vitamin D analogues calcipotriene and calcitriol can improve psoriasis, but they tend to work very slowly. Some irritation can occur, but serious adverse effects (such as hypercalcemia) are rare and only seen with heavy use (> 100 g/wk).12 Topical corticosteroids are used in combination with vitamin D preparations to speed the rate of disease improvement and to reduce irritation. The use of vitamin D preparations with corticosteroids may help reduce how much topical corticosteroid is needed for disease control.
Tazarotene is a topical retinoid that also can be used for psoriasis in combination with topical corticosteroids; however, it is less effective and more irritating than topical vitamin D.13 Tazarotene has a teratogenic effect; therefore, pregnancy must be avoided. Application site burning and itching are common adverse effects.12
Targeted phototherapy/laser therapy is effective but is perhaps less convenient than topical treatment for most patients. Laser therapy is preferred over whole-body therapy for localized psoriasis, since it spares the uninvolved skin from UV radiation and allows higher doses to be used, speeding the response to treatment and reducing the risk of treatment.
Topical immunomodulators such as tacrolimus and pimecrolimus, while not approved by the U.S. Food and Drug Administration for the treatment of psoriasis, are used with good success on sensitive skin sites such as the face and genital area. They can cause stinging when they are first used. Unlike topical corticosteroids, immunomodulators do not have the adverse effect of skin changes such as atrophy, telangiectasia, or permanent purple striae.14
Over-the-counter coal tar formulations once were commonly recommended, but they are messy. Anthralin is no longer used much because of its staining properties, including of ceramic sinks and tubs.
Extensive psoriasis. Phototherapy is recommended as a first-line therapy for moderate to severe psoriasis. Medically supervised in-office phototherapy is considered the preferred approach to assure safety; however, many patients cannot adhere to this regimen secondary to financial, travel, or time restrictions. Home phototherapy with a prescription home phototherapy device is another option. Sunlight works, as well. Tanning beds are easily accessible in most neighborhoods and offer an alternative way of accessing phototherapy (although some dermatologists and organizations discourage their use). While tanning beds emit primarily UVA radiation and have a wide-spectrum distribution of UV output that is poorly regulated and not standardized, they still are an effective form of psoriasis treatment.15
Office phototherapy uses mainly UVB, particularly “narrow-band” UVB. Psoralen plus UVA (PUVA) is a combination therapy in which an oral agent (psoralen) is used to increase the tissue’s response to the UV radiation treatment. If not adequately monitored and controlled, this combination can result in rare but life-threatening burns.
Before the initiation of UV treatment, an initial skin examination can be done, since phototherapy, especially PUVA, can lead to subsequent development of skin cancers.16 An ophthalmologic examination also is warranted for patients receiving PUVA. Patients should wear UV-blocking goggles during phototherapy for eye protection (and for the duration of time that psoralen is in the body during PUVA treatments). Phototherapy has good efficacy and a good cost to benefit ratio.16 Long-term effects of high, cumulative doses of UV exposure can lead to erythema from overexposure in the short run, and over time, to premature skin aging and development of skin cancers. The safety and efficacy of phototherapy, used in conjunction with other therapies, is still being studied.17
Oral agents. Methotrexate is an antimetabolite used in the long-term therapy of psoriasis. Because of its low cost, it usually is the first systemic therapy used in psoriasis patients who need systemic treatment. It has reasonable efficacy, but it can cause severe acute (pancytopenia) and chronic (hepatotoxicity, pulmonary toxicity) adverse effects. Patients need to be screened for alcohol abuse and hepatic disease. The NPF offers a helpful resource for educating patients about methotrexate and other systemic psoriasis treatments.18
Acitretin is a vitamin A derivative that is used to treat palmoplantar and pustular psoriasis, as well as erythrodermic psoriasis.19 While not particularly effective by itself for plaque psoriasis, acitretin is synergistic with all forms of phototherapy for psoriasis and makes phototherapy more effective. Acitretin is not particularly immunosuppressive and is not associated with an increased risk of opportunistic infections. Acitretin is a potent teratogen and should not be used in women of childbearing potential. Doses of 25 mg every other day to 50 mg daily can be used. Monitoring acitretin use (as with isotretinoin) includes liver function tests and triglyceride level assessment at baseline, then monthly until stable, and then every 6 months thereafter.
Before the development of more recent therapies, cyclosporine had been used for the treatment of severe, acute psoriasis in doses of 2.5 to 4 mg/kg/d. Long-term renal toxicity limits its value as a psoriasis treatment, however.
Apremilast is an oral phosphodiesterase-4 inhibitor used in the treatment of moderate to severe plaque psoriasis, including nail, scalp, and palmoplantar manifestations, enthesitis, and dactylitis. The medication is generally well tolerated, with the adverse effects of generally transient nausea and diarrhea in 15% to 20% of patients.20

Biologic therapies inhibit specific cytokines such as TNF-α, IL-17, and IL-23 that play a critical role in the course of psoriasis development (Table 5). These drugs are highly effective. Adalimumab was considerably more effective than methotrexate in a head-to-head trial.21 Based on clinical trials, secukinumab (which inhibits IL-17) and infliximab seem to be the most potent treatments, with adalimumab and ustekinumab (which inhibits IL-23) the next most effective, and etanercept the least effective of the biologics but still more potent than apremilast. The Psoriasis Longitudinal Assessment and Registry (PSOLAR) enrolled patients on both biologic and nonbiologic treatments and found excellent safety for biologics, with serious infection rates lowest for ustekinumab, roughly similar for etanercept vs no biologic, and slightly higher for adalimumab and infliximab.21,22
Future developments. New systemic formulations that are now being studied demonstrate good efficacy and a low adverse-effect profile (Table 6). However, long-term, prospective studies are needed to establish long-term safety and efficacy.
Emerging topical preparations for the treatment of psoriasis include vitamin D3 derivatives, combined vitamin D3 derivatives and corticosteroids, salicylic acid and corticosteroids, nortriptyline-containing compounds, new steroidal agents, agents that block neurogenic inflammation, new phosphodiesterase inhibitors, janus kinase inhibitors, nonsteroidal anti-inflammatory drugs, topical calcineurin inhibitors, antiproliferative agents, and coal tar formulations.23

Primary Care Provider Role
Psoriasis is a common condition that primary care providers will see often. The primary care provider will treat many patients exclusively, while others may be managed in partnership with a dermatologist and a rheumatologist.
Psoriasis, among other immune conditions, is associated with an increased risk of cardiovascular disease and obesity.11,24 The primary care providers caring for patients with psoriasis are well positioned to implement strategies for risk-factor modification; these measures already are part of daily primary care practice. Counseling about smoking cessation, weight maintenance, exercise, and normal blood pressure are recommended for all patients in general and are especially applicable to patients with psoriasis. Other risk factors include insulin resistance (treated with anti-inflammatory and biological agents) and hyperhomocysteinemia (treated with folic acid supplementation, especially when methotrexate is used); any additional prothrombotic risk factor usually is treated with low-dose aspirin or another method of anticoagulation.11 Other associated comorbidities include depression (with up to 60% prevalence), immune-mediated diseases (such as Crohn disease, ulcerative colitis, and multiple sclerosis), and malignancies (such a lymphoma and squamous cell carcinomas).25
Table 7 summarizes the screening tests that are recommended for the various biologic agents being used as psoriasis therapy.26

Referral to a dermatologist is warranted whenever the primary care provider believes that the patient would benefit from specialist expertise. This is based on providers’ comfort level in treating patients with psoriasis, their understanding of the drug mechanisms and adverse-effect profile, and, most importantly, previous clinical experience. The decision to refer often depends on geographic location and the availability of the specialist. Many primary care providers feel very comfortable continuing to manage a patient whose treatment has been implemented by a dermatologist. Often, all that is required is clear, regular communication between the 2 providers. From a patient’s perspective, this may translate into cost savings (depending on copayments applied and distance traveled) and, most importantly, an increase in patient satisfaction.
Simona Bartos, MPH, BS, is at the Center for Dermatology Research in the Department of Dermatology at the Wake Forest University School of Medicine in Winston-Salem, North Carolina.
Dane Hill, MD, is at the Center for Dermatology Research in the Department of Dermatology at the Wake Forest University School of Medicine in Winston-Salem, North Carolina.
Steven R. Feldman, MD, PhD, is at the Center for Dermatology Research in the Department of Dermatology, the Department of Pathology, and the Department of Public Health Sciences at the Wake Forest University School of Medicine in Winston-Salem, North Carolina.
Disclosures
The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories.
Steven R. Feldman, MD, PhD, is a speaker for Janssen and Novartis. He has received grants from Galderma Laboratories, Janssen, AbbVie, Amgen, Stiefel Laboratories/GlaxoSmithKline, Celgene, and Anacor Pharmaceuticals. He is a consultant for Amgen, Baxter, Caremark, Gerson Lehrman Group, Guidepoint, HanAll Pharmaceutical, Eli Lilly, Merck, Mylan, Novartis, Pfizer, Qurient, Suncare Research Laboratories, and XenoPort. He is the founder of and holds stock in Causa Research, and he holds stock in and is majority owner of Medical Quality Enhancement Corp. He receives Royalties from UpToDate and Xlibris.
Simona Bartos, MPH, BS, and Dane Hill, MD, have no relationships to disclose.
References:
- Lebwohl M. Psoriasis. Lancet. 2003;361(9364): 1197-1204.
- Rapp SR, Feldman SR, Exum ML, Fleischer AB Jr, Reboussin DM. Psoriasis causes as much disability as other major medical diseases. J Am Acad Dermatol. 1999;41(3 pt 1):401-407.
- Finlay AY, Khan GK, Luscombe DK, Salek MS. Validation of Sickness Impact Profile and Psoriasis Disability Index in psoriasis. Br J Dermatol. 1990;123(6):751-756.
- Dubertret L, Mrowietz U, Ranki A, et al; EUROPSO Patient Survey Group. European patient perspectives on the impact of psoriasis: the EUROPSO patient membership survey. Br J Dermatol. 2006;155(4):729-736.
- Schön MP, Boehncke W-H. Psoriasis. N Engl J Med. 2005;352(18):1899-1912.
- Mrowietz U, Reich K. Psoriasis—new insights into pathogenesis and treatment. Dtsch Arztebl Int. 2009;106(1-2):11-19.
- Griffiths CEM, Barker JNWN. Pathogenesis and clinical features of psoriasis. Lancet. 2007; 370(9583):263-271.
- Fortune DG, Richards HL, Griffiths CEM. Psychologic factors in psoriasis: consequences, mechanisms, and interventions. Dermatol Clin. 2005; 23(4):681-694.
- Xhaja A, Shkodrani E, Frangaj S, Kuneshka L, Vasili E. An epidemiological study on trigger factors and quality of life in psoriatic patients. Mater Sociomed. 2014;26(3):168-171.
- Veale DJ. Psoriatic arthritis: recent progress in pathophysiology and drug development. Arthritis Res Ther. 2013;15(6):224.
- Kaplan MJ. Cardiometabolic risk in psoriasis: differential effects of biologic agents. Vasc Health Risk Manag. 2008;4(6):1229-1235.
- Weigle N, McBane S. Psoriasis. Am Fam Physician. 2013;87(9):626-633.
- Menter A, Korman NJ, Elmets CA, et al; American Academy of Dermatology. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 3: guidelines of care for the management and treatment of psoriasis with topical therapies. J Am Acad Dermatol. 2009; 60(4):643-659.
- du Vivier A, Stoughton RB. Tachyphylaxis to the action of topically applied corticosteroids. Arch Dermatol. 1975;111(5):581-583.
- Radack KP, Farhangian ME, Anderson KL, Feldman SR. A review of the use of tanning beds as a dermatological treatment. Dermatol Ther (Heidelb). 2015;5(1):37-51.
- Nast A, Kopp I, Augustin M, et al. German evidence-based guidelines for the treatment of psoriasis vulgaris (short version). Arch Dermatol Res. 2007;299(3):111-138.
- LeVine MJ, Parrish JA. The effect of topical fluocinonide ointment on phototherapy of psoriasis. J Invest Dermatol. 1982;78(2):157-159.
- National Psoriasis Foundation. Systemic Medications for Psoriasis and Psoriatic Arthritis Including Biologics and Oral Treatments. Portland, OR: National Psoriasis Foundation; 2015. https://www.psoriasis.org/sites/default/files/systemics_booklet.pdf. Accessed February 2, 2016.
- Kuijpers ALA, van Dooren-Greebe JV, van de Kerkhof PCM. Failure of combination therapy with acitretin and cyclosporin A in 3 patients with erythrodermic psoriasis. Dermatology. 1997;194(1):88-90.
- Deeks ED. Apremilast: a review in psoriasis and psoriatic arthritis. Drugs. 2015;75(12):1393-1403.
- Kalb RE, Fiorentino DF, Lebwohl MG, et al. Risk of serious infection with biologic and systemic treatment of psoriasis: results from the Psoriasis Longitudinal Assessment and Registry (PSOLAR). JAMA Dermatol. 2015;151(9):961-969.
- Aslam A, Griffiths CEM. Drug therapies in dermatology. Clin Med (Lond). 2014;14(1):47-53.
- Chiricozzi A, Pitocco R, Saraceno R, Nistico SP, Giunta A, Chimenti S. New topical treatments for psoriasis. Expert Opin Pharmacother. 2014; 15(4):461-470.
- Debbaneh M, Millsop JW, Bhatia BK, Koo J, Liao W. Diet and psoriasis, part I: impact of weight loss interventions. J Am Acad Dermatol. 2014; 71(1):133-140.
- Gottlieb A, Korman NJ, Gordon KB, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 2: psoriatic arthritis: overview and guidelines of care for treatment with an emphasis on the biologics. J Am Acad Dermatol. 2008;58(5):851-864.
- Ahn CS, Dothard EH, Garner ML, Feldman SR, Huang WW. To test or not to test? An updated evidence-based assessment of the value of screening and monitoring tests when using systemic biologic agents to treat psoriasis and psoriatic arthritis. J Am Acad Dermatol. 2015;73(3): 420-428.e1.