
Lyme Disease
A 44-year-old man presented to an urgent care clinic in Western Iowa with a complaint of generalized fatigue, malaise, and subjective fevers of 3 weeks’ duration. He had noticed a rash on the right side of his waist 4 days before presentation. The rash did not itch and was not painful. He denied joint pain or swelling, palpitations, shortness of breath, and upper respiratory or gastrointestinal symptoms. On inquiry about travel, he mentioned that he had been on a vacation in Northern Wisconsin approximately 1 month prior and had had at least 1 tick bite during that time.
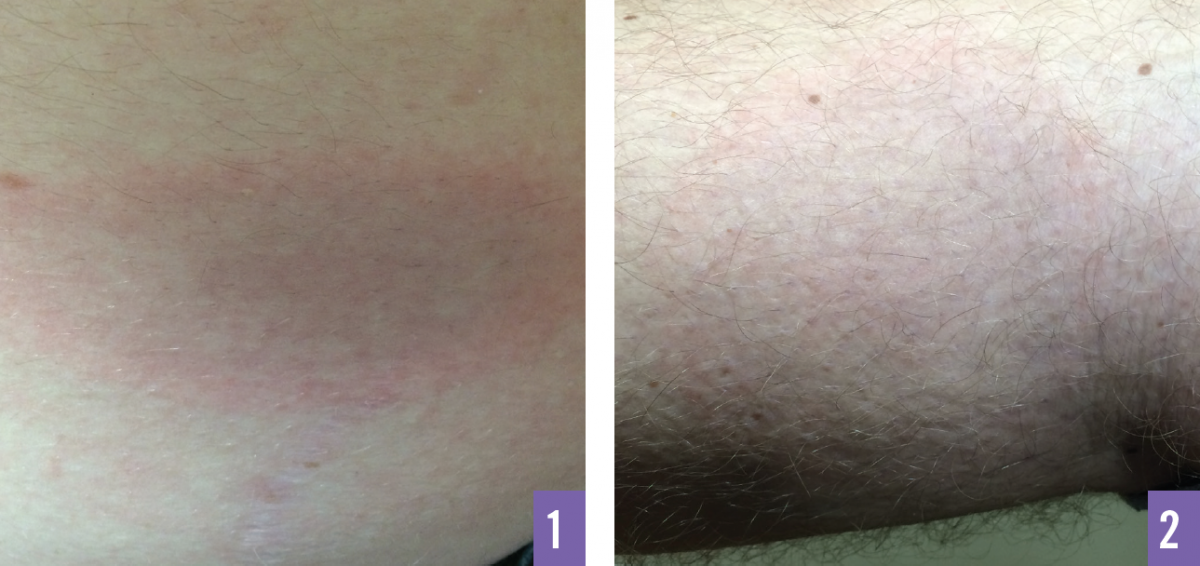
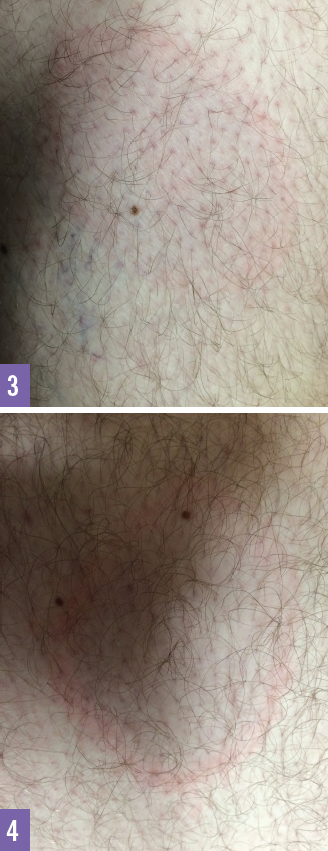
Physical examination. Examination of the skin was positive for 4 lesions, one on the right flank and the others on the lower extremities. The lesions were ovoid, erythematous, and slightly raised. The lesion on the flank featured central clearing, and the erythema had assumed a bull’s-eye appearance. No warmth or tenderness were noted on palpation of the rash. Vital signs and musculoskeletal and cardiac examination findings were normal.
Diagnosis and treatment. The patient received a presumptive diagnosis of Lyme disease and was started on a regimen of doxycycline. Six days later, serology test results returned positive for immunoglobulin M antibodies against Borrelia burgdorferi by western blot test.
Discussion. Lyme disease is a very common cause of erythema migrans (EM).1,2 Lyme disease is caused by spirochete B burgdorferi and is transmitted by Ixodes ticks.1 Rodents such as the white-footed mouse are the primary reservoirs of Borrelia spirochete species.
Lyme disease is the most common tickborne disease in the United States.1 The risk for contracting Lyme disease is highest in Connecticut, Delaware, Maine, Maryland, Massachusetts, Minnesota, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Wisconsin.1
The incidence of Lyme disease is highest among children from 5 to 14 years of age and adults from 40 to 50 years of age.2 Ticks ingest the nymphal stage of the spirochete from an infected animal and transfer the disease to humans.2 Infection occurs primarily during the late spring and summer months, when nymphs are most active.1 The peak incidence of EM also is during spring and summer.2
During the initial days after tick exposure, Lyme disease can present with nonspecific signs and symptoms resembling a viral syndrome, such as fatigue, anorexia, headache, myalgia, and fever. These manifestations can occur up to 30 days after a tick bite.1 Upper respiratory and gastrointestinal signs and symptoms are uncommon in Lyme disease.
Early localized disease is characterized by the appearance of the characteristic skin lesion, EM, and other nonspecific symptoms. Approximately 80% of patients develop EM at the site of the tick bite, usually within 7 to 14 days and up to 30 days after having been bitten.1 The rash often is found in or near the axillae, groin, waist, back, and legs.2
EM classically is reported as single lesion, appearing as a uniform, erythematous, oval to circular lesion with a median diameter of 16 cm.1 The rash is not particularly painful, but occasionally it may burn or itch and often feels hot to the touch. The lesion typically expands slowly over the course of days or weeks, often with central clearing, and may reach a diameter of more than 20 cm. After central clearance, the lesion may develop a more complex target-like or bull’s-eye appearance. EM lesions rarely have necrotic or vesicular centers. Histologic examination shows vascular endothelial cell injury.
Early disseminated Lyme disease can occur days to weeks after having sustained a tick bite. The appearance of multiple EM lesions is the most common presentation of disseminated disease.2 The most common sites of extracutaneous involvement are the joints, nervous system, and cardiovascular system.1 Neurologic involvement occurs in 15% of patients and can include meningitis, radiculopathy, facial nerve palsy, and peripheral neuropathy.1 Lyme carditis occurs in approximately 4% to 10% of patients and may present as chest pain, dyspnea on exertion, palpitations, and some form of atrioventricular block.1
Late Lyme disease may occur months to a few years after the onset of infection and may not be preceded by a history of disseminated Lyme disease. Arthritis in 1 or more joints is the most common feature of late Lyme disease.1 In some patients, subjective symptoms of arthralgia, myalgia, and fatigue persist for weeks to months after treatment. These cases are classified as posttreatment Lyme disease syndrome if they are disabling and persist for 6 months or longer.2
Serologic testing for anti-B burgdorferi antibodies is recommended for patients with disseminated disease. Immunoglobulins M and G are detected by enzyme-linked immunosorbent assay and confirmed by western blot testing. The Centers for Disease Control and Prevention recommends 2-tier testing.1 Based on symptoms at presentation, a complete blood cell count, metabolic panel, electrocardiography, and lumbar puncture may be necessary.
Treatment for Lyme disease is mainly based on clinical manifestations. Oral antibiotic therapy is recommended for localized disease. Intravenous antibiotic therapy is reserved for patients with neurologic symptoms, cardiac involvement, or refractory arthritis.1 The drugs of choice for oral therapy are doxycycline (100 mg twice daily), amoxicillin (500 mg thrice daily), and cefuroxime (500 mg twice daily). Doxycycline is the recommended first-line agent because of its activity against other tickborne illnesses.1 The recommended duration of therapy is 21 days. The recommended intravenous regimens are ceftriaxone (2 g once daily), cefotaxime (2 g every 8 h) or penicillin G (24 million units daily).1,2
Avoidance of tick-infested areas, application of 20% DEET, and covering the skin with long pants and long-sleeve shirts are effective in preventing tick bites.2 Performing tick checks and bathing within 2 hours of outdoor activity has been shown to reduce the risk of infection.1 Removal of ticks within 24 hours also prevents acquisition of Lyme disease. A single 200-mg dose of oral doxycycline is recommended as prophylaxis for adults within 72 hours of tick removal.1
References:
- Wright WF, Riedel DJ, Talwani R, Gilliam BL. Diagnosis and management of Lyme disease. Am Fam Physician. 2012;85(11):1086-1093.
- Shapiro ED. Lyme disease. N Engl J Med. 2014;370(18):1724-1731.